What Every Oncologist Needs to Know About CAR-T Toxicity
A Community Practice Guide
CAR T-cell therapy has transformed the treatment of relapsed and refractory hematologic malignancies, but the toxicity profile increasingly intersects with community oncology. With eight products now approved across CD19- and BCMA-directed indications, and with bridging, lymphodepletion, and post–day-30 surveillance routinely delivered locally, the community physician carries most of the journey. The toxicities most likely to drive non-relapse mortality — late infections, prolonged cytopenias, immune effector cell–associated enterocolitis, and delayed neurotoxicity — present weeks to months after the patient has left the CAR-T center.
The Construct Is the Cause
The most important concept in CAR-T toxicity is that the construct itself is the cause. A native T cell requires two independent signals to activate: signal 1, the T-cell receptor engaging an antigenic peptide on MHC; and signal 2, a separate co-stimulatory receptor engaging its ligand on the target cell. Both must arrive together; signal 1 alone drives the T cell into anergy. This two-signal architecture is a safety mechanism that prevents indiscriminate activation against self. Tumors exploit it — many fail to provide co-stimulation, and many down-regulate MHC.
The CAR construct solves both problems at once. The native TCR is replaced with an antibody-derived scFv that binds the target directly, MHC-independently. The co-stimulatory domain — CD28 or 4-1BB — is fused intracellularly behind the scFv alongside CD3-zeta, so one binding event delivers both signals. The native safety check is collapsed into a single recognition step. That is the source of CAR-T potency, and it is the source of every toxicity that follows. Two consequences flow directly from the design. Antibody-like, MHC-independent recognition means any tissue expressing the target antigen is at risk — the basis of B-cell aplasia, hypogammaglobulinemia, and the late friendly-fire syndromes. And because co-stimulation is hard-wired, the construct can signal tonically. CD28 produces rapid, high-magnitude activation with an early cytokine surge; 4-1BB signals through nuclear factor κB more slowly — lower peak inflammation, longer biological tail.
A Tale of Two Halves
CAR-T toxicity falls into two phases at roughly day 30. The first 30 days are cytokine-driven: cytokine release syndrome (CRS, IL-6, days 1–14), immune effector cell–associated neurotoxicity syndrome (ICANS, IL-1 and IFN-γ, days 2–14), and IEC-associated hemophagocytic lymphohistiocytosis–like syndrome (IEC-HS, IL-1 and IFN-γ, days 7–21). After day 30, the dominant toxicities are direct on-target off-tumor effects: hematotoxicity (ICAHT), late infections, non-ICANS neurotoxicity, and IEC-enterocolitis. The patient is in the community by then. The bedside rule: match the treatment to the cytokine driver.
CRS: IL-6, days 1–14
CRS cannot be present without fever — that is the anchor. ASTCT 2019 grades severity by the worst single domain of fever, hypotension, and hypoxia. Grade 1 (fever only) is supportive care; consider tocilizumab 8 mg/kg if fever persists beyond 24–72 hours. Grade 2 (fluid-responsive hypotension or low-flow oxygen): tocilizumab plus dexamethasone 10 mg q12h if hypotension persists. Grade 3 (vasopressor or high-flow oxygen): tocilizumab plus dexamethasone 10 mg q6h. Grade 4 (multiple vasopressors or ventilator): tocilizumab plus methylprednisolone 500 mg–1 g IV twice daily. Tocilizumab does not appear to abrogate efficacy and is the cornerstone.
Onset varies by construct. CD28 products (axi-cel, brexu-cel) produce CRS with median onset around day 2; 4-1BB products (cilta-cel, tisa-cel, liso-cel, obe-cel) onset later, median day 7. A day-7 fever in a CD28 recipient is more likely infectious; the same fever after 4-1BB should prompt active CRS consideration. Obe-cel, approved November 2024 for adult R/R B-cell ALL with severe CRS in only 2–3% of patients, is also the first CAR T-cell therapy approved without a REMS requirement — a regulatory signal of growing comfort with decentralized monitoring.
IEC-HS: The Great Imitator
IEC-HS is the toxicity most often missed in the community, because it mimics CRS but requires a different treatment. The distinguishing feature: in CRS, IL-6 is elevated; in IEC-HS, IL-6 drops while ferritin continues to climb. Fever plus rising ferritin (especially >10,000 ng/mL), rising LFTs, and coagulopathy — that is IEC-HS, not CRS. Incidence is 5–10% with BCMA products (median day 9) and 1–3% with CD19 products; historical mortality is 20–40%. The strongest single predictor is failure of CRS to resolve — persistent fever beyond 72 hours despite tocilizumab.
The treatment principle: stop tocilizumab monotherapy. IL-6 is not the driver, and continuing toci may obscure the C-reactive protein trend. Anakinra 100–200 mg IV every 6–12 hours plus methylprednisolone 1 g/day × 3 days is the backbone. Second-line salvage is emapalumab (anti–IFN-γ), mechanistically rational because IFN-γ is central; ruxolitinib (JAK1/2) is an alternative. Refractory, life-threatening cases warrant HLH-94 etoposide-based regimens with adult HLH expertise.
ICANS: The Fog
Cytokines (principally IL-1 and GM-CSF) breach the blood–brain barrier and provoke microglial neurotoxicity. CD28 products produce any-grade ICANS in 60–65% (≥G3 in 25–30%, median day 5); 4-1BB products in 20–30% (≥G3 in 5–12%, median day 7–9). Bedside assessment is the 10-point ICE score (orientation, naming three objects, command-following, writing a standard sentence, counting backwards from 100 by 10s). Grading is set by the worst single domain across ICE score, level of consciousness, seizures, motor findings, and cerebral edema — deep focal weakness and edema on imaging auto-grade to 4.
Treatment escalates from levetiracetam prophylaxis and neuro checks at grade 1, to dexamethasone 10 mg IV q6h at grade 2, to methylprednisolone 1 mg/kg q12h with ICU transfer at grade 3, to high-dose methylprednisolone 1 g/day at grade 4 with anakinra 200 mg IV q6h for refractory disease. The cardinal rule: do not use tocilizumab for isolated ICANS. It is a large molecule that does not cross the blood–brain barrier, and use without concurrent CRS can paradoxically increase systemic IL-6. Dexamethasone is the cornerstone. The principal modifiable risk factor is tumor burden; bridging radiotherapy for tumors >5 cm reduces grade ≥3 CRS from ~13% to ~7%, and prophylactic dexamethasone on days 0–2 (ZUMA-1 Cohort 6) dropped grade ≥3 CRS from 13% to 0% and ICANS from 28% to 15% without compromising response.
ICAHT (Prolonged Cytopenias): The Drought
Hematotoxicity is the dominant long-tail toxicity. Three mechanisms operate together: cytokine suppression of hematopoietic stem cells (early ICAHT), niche injury from lymphodepletion and the cytokine storm (late ICAHT after day 30), and unmasking of pre-existing TET2 or DNMT3A clones (the aplastic phenotype, highest non-relapse mortality). Three recovery patterns: quick recovery by day 21; intermittent with a redip around day 14; and aplastic. The CAR-HEMATOTOX score, calculated before lymphodepletion from ferritin, CRP, ANC, platelets, and hemoglobin, predicts severe or prolonged neutropenia in ~60% of high-risk patients versus ~8% of low-risk. G-CSF, historically held out of concern for exacerbating CRS, does not worsen severe CRS or ICANS in current evidence and should be started at day +2 or later when the ANC is below 500/μL — and can be initiated earlier in CAR-HEMATOTOX high-risk patients who have not developed CRS. Grade 4 aplastic ICAHT lasting beyond 30 days warrants an autologous CD34+ stem cell boost — which is why collecting stem cells before CAR-T referral is a meaningful upstream intervention community oncologists can champion.
Infection: The Siege
Infection risk reflects a multilayered immune defect: lymphodepletion, B-cell aplasia, hypogammaglobulinemia, prolonged neutropenia, and steroid- and tocilizumab-related T-cell dysfunction. Risk runs in three phases. Early (day 0–30): bacterial > viral, mostly bloodstream and pneumonia. Intermediate (day 30–90): viral reactivation (CMV, HHV-6, HSV) and fungal — community-managed. Late (day 90+): opportunistic and encapsulated organisms, driven by persistent hypogammaglobulinemia. Standard prophylaxis is acyclovir for HSV/VZV, TMP-SMX for PJP, fluconazole or mold coverage for prolonged neutropenia, IVIG when IgG falls below 400 mg/dL, and CMV/EBV/HBV PCR monitoring through the first 90 days. Fever may be masked by tocilizumab and steroids; rule out infection before attributing fever to CRS, particularly after day 14.
Non-ICANS Neurotoxicity: Friendly Fire
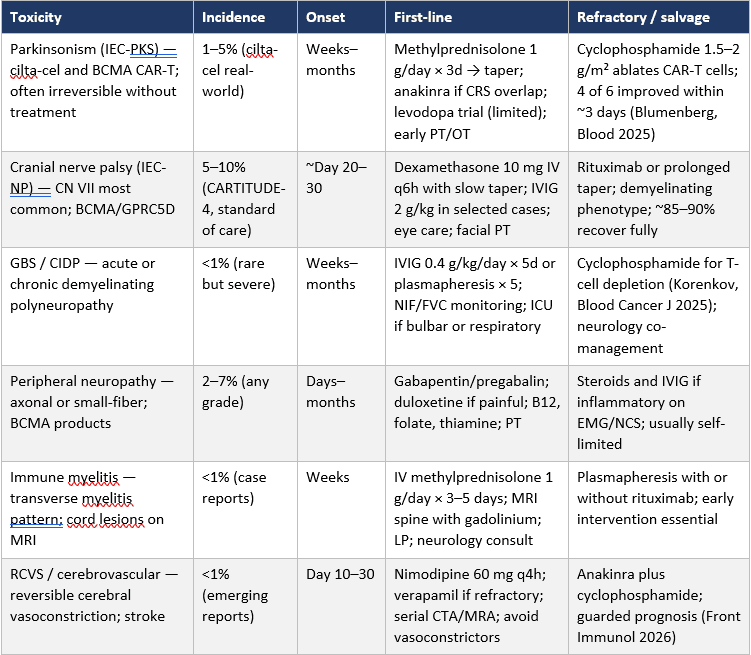
These syndromes emerge weeks to months after infusion and are not captured by the ICE score. The illustrative case is the 62-year-old man on day 42 after BCMA CAR-T with new gait disturbance, parkinsonian features, and cognitive blunting — too late for ICANS, the wrong phenotype for IEC-HS. The most clinically significant manifestation is parkinsonism (IEC-PKS, 1–5% of cilta-cel recipients), often irreversible without treatment. Cyclophosphamide 1.5–2 g/m² IV × 1 ablates the responsible CAR-T cells; in the Blumenberg series (Blood 2025), four of six steroid-refractory IEC-PKS patients improved within ~3 days, with the antimyeloma response preserved out to 21 months. Other late neurotoxicities — cranial nerve palsies (CN VII most common, 5–10% with cilta-cel and GPRC5D agents), GBS/CIDP, peripheral neuropathy, transverse myelitis — generally respond to a short course of steroids in 85–90% of cases. A normal ICE score in a patient with new gait disturbance or progressive cognitive change after BCMA CAR-T is not reassurance.
IEC-Associated Enterocolitis: The Late, Often-Missed Friendly-Fire Syndrome
IEC-enterocolitis is a late, often-fatal toxicity that occurs when CAR-T cells infiltrate gut mucosa. In the US Multiple Myeloma Immunotherapy Consortium series of 1,287 BCMA CAR-T infusions (Nadeem, Blood Cancer J 2024), incidence was 1.2%, with a roughly tenfold disparity between products: 0.2% with ide-cel versus 2.2% with cilta-cel. Median onset was day 79–92 (range 22–210) — well past the REMS window. Mortality was 36%. Presentation is acute, high-volume, non-bloody diarrhea with a negative infectious workup; biopsy shows a GVHD-like pattern with CAR+ T cells in the lamina propria. Steroids first (prednisone 1 mg/kg; ~40% respond; budesonide can bridge), then infliximab 5 mg/kg if no response within 3–5 days (~50% of steroid-refractory respond), then vedolizumab 300 mg (~33%). Send T-cell clonality on the biopsy; T-cell lymphoproliferative disorder must be excluded.
Secondary T-Cell Malignancy: The FDA Class Warning
In November 2023, the FDA opened a safety investigation after FAERS flagged T-cell lymphomas — some containing the CAR transgene — in CAR-T recipients. The investigation culminated in an April 2024 class-wide boxed warning applied to all approved products, with lifelong monitoring required and 15-year post-marketing follow-up mandated. The data converge on a low but real absolute risk: 4.3% of FAERS adverse-event reports (Elsallab, Blood 2024) include any second primary malignancy, with T-cell and myeloid neoplasms disproportionately represented. Single-institution series put any-secondary-cancer incidence at ~3.6% (Penn, 16/449), with only 1 T-cell lymphoma; Stanford identified 1 T-cell lymphoma in 724 patients, and it did not contain the CAR transgene. Any new lymphoproliferative process post-CAR-T requires biopsy with T-cell receptor clonality and CAR-transgene PCR, with pathology alerted to the post-CAR-T context. The same workflow covers the IEC-enterocolitis biopsy. Lifelong monitoring belongs in the survivorship care plan.
Conclusion
CAR-T cell therapy no longer begins and ends at the CAR-T center. The toxicities most likely to drive non-relapse mortality present to community physicians during exactly the phase when the patient has come home. Recognition rests on three habits: knowing the time window, knowing the construct, and matching therapy to the cytokine driver. Tocilizumab is for CRS, not for IEC-HS or isolated ICANS. Anakinra and steroids are the backbone of IEC-HS and of refractory ICANS. G-CSF is safe and underused in ICAHT. Late non-bloody diarrhea after BCMA CAR-T requires biopsy and a low threshold for infliximab. Delayed gait or cognitive change after cilta-cel may be parkinsonism that responds to cyclophosphamide. With these patterns in hand, the community physician is positioned to make the catch that the CAR-T center cannot — because, by then, the patient is no longer there.
Practice Takeaways
- No fever, no CRS. Fever is the anchor.
- Construct predicts onset. Day-2 fever after CD28 reads differently from day-7 fever after 4-1BB.
- Don't use tocilizumab for IEC-HS or isolated ICANS. IL-6 isn't the driver of either.
- Anakinra plus steroids are the backbone of IEC-HS and refractory ICANS.
- Prophylactic dexamethasone (days 0–2) drops severe CRS and ICANS without compromising response.
- G-CSF is safe and accelerates neutrophil recovery; can be initiated earlier in CAR-HEMATOTOX high-risk patients without active CRS.
- Collect stem cells before CAR-T. They are the definitive intervention for grade 4 aplastic ICAHT.
- A normal ICE score does not exclude late neurotoxicity. New gait disturbance or cognitive change after BCMA CAR-T needs a separate workup.
- Lifelong monitoring for secondary T-cell malignancy. New lymphoproliferative findings require biopsy with clonality and CAR-transgene PCR.
Key References
1. Lee DW, et al. ASTCT consensus grading for CRS and neurologic toxicity. Biol Blood Marrow Transplant. 2019;25:625–638.
2. Hines MR, et al. IEC-HS criteria and management. Transplant Cell Ther. 2023.
3. Rejeski K, et al. ICAHT: EHA/EBMT consensus grading. Blood. 2023.
4. Strati P, et al. Prophylactic corticosteroids for CRS in axi-cel (ZUMA-1 Cohort 6). Blood Adv. 2021.
5. Roddie C, et al. Obecabtagene autoleucel in R/R B-cell ALL (FELIX). N Engl J Med. 2024.
6. Blumenberg V, et al. Cyclophosphamide for refractory cilta-cel parkinsonism. Blood. 2025;145:2788.
7. Nadeem O, et al. IEC-enterocolitis after BCMA CAR T-cell therapy. Blood Cancer J. 2024;14:194.
8. Verdun N, Marks P. Secondary cancers after CAR T-cell therapy. N Engl J Med. 2024;390:584–586.
9. Elsallab M, et al. Second primary malignancies after commercial CAR T-cell therapy: FAERS analysis. Blood. 2024;143:2099–2105.
10. NCCN. Management of Immunotherapy-Related Toxicities. Available at: nccn.org.
Originally presented at the Binaytara Cellular Therapy Symposium 2026, Session 5: Cellular Therapy for Community Practice.
Supplementary Materials | Tables
Reference Tables for CAR-T Cell Therapy Toxicity Management
Nine tables covering products, grading systems, and management algorithms
Table 1. FDA-Approved CAR T-Cell Products (2026)
Eight products approved across CD19- and BCMA-directed indications. Toxicity rates vary substantially by product and largely track with the choice of co-stimulatory domain. Obe-cel (Aucatzyl), approved November 2024, is the first CAR T-cell therapy approved by the FDA without a Risk Evaluation and Mitigation Strategy (REMS) requirement.
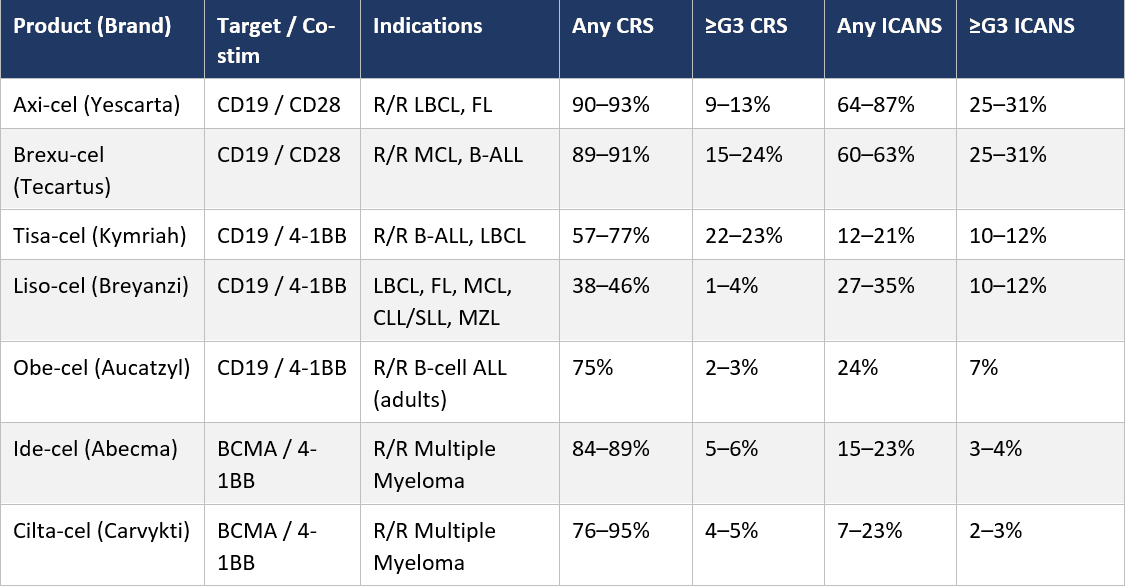
Table 2. ASTCT 2019 Consensus Grading and Management of CRS
Cytokine release syndrome (CRS) cannot be present without fever. Grade is assigned by the worst single domain across fever, hypotension, and hypoxia. Tocilizumab is the cornerstone of grade ≥2 management; steroids are escalated in parallel.Table 3. ASTCT IEC-HS Diagnostic Criteria and Management (Hines 2023)
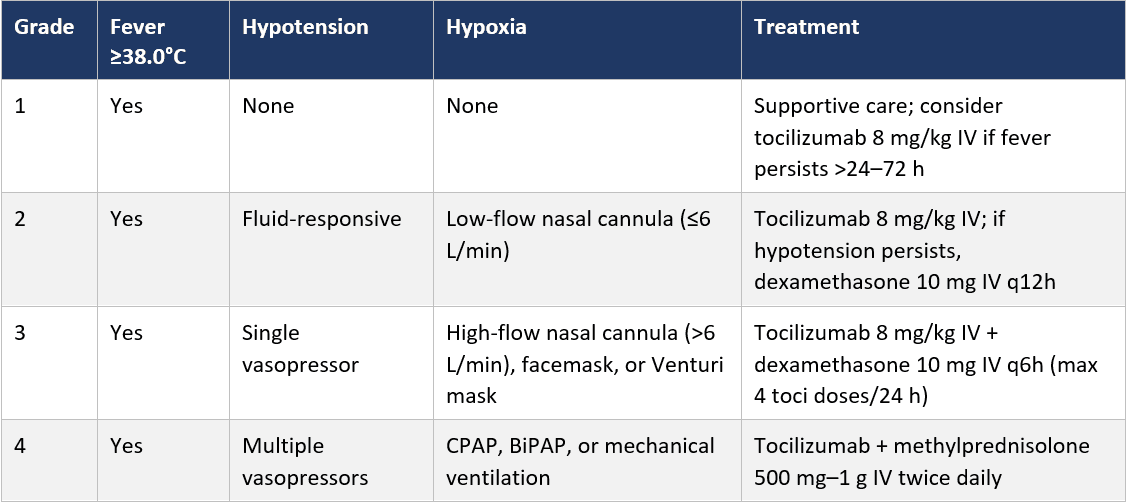
Table 3. ASTCT IEC-HS Diagnostic Criteria and Management (Hines 2023)
Immune effector cell–associated hemophagocytic lymphohistiocytosis–like syndrome (IEC-HS) is driven by IFN-γ and IL-1, not IL-6. Diagnosis requires rising ferritin plus involvement of two or more organ systems. The treatment principle is to stop tocilizumab monotherapy and switch to anakinra plus high-dose steroids.
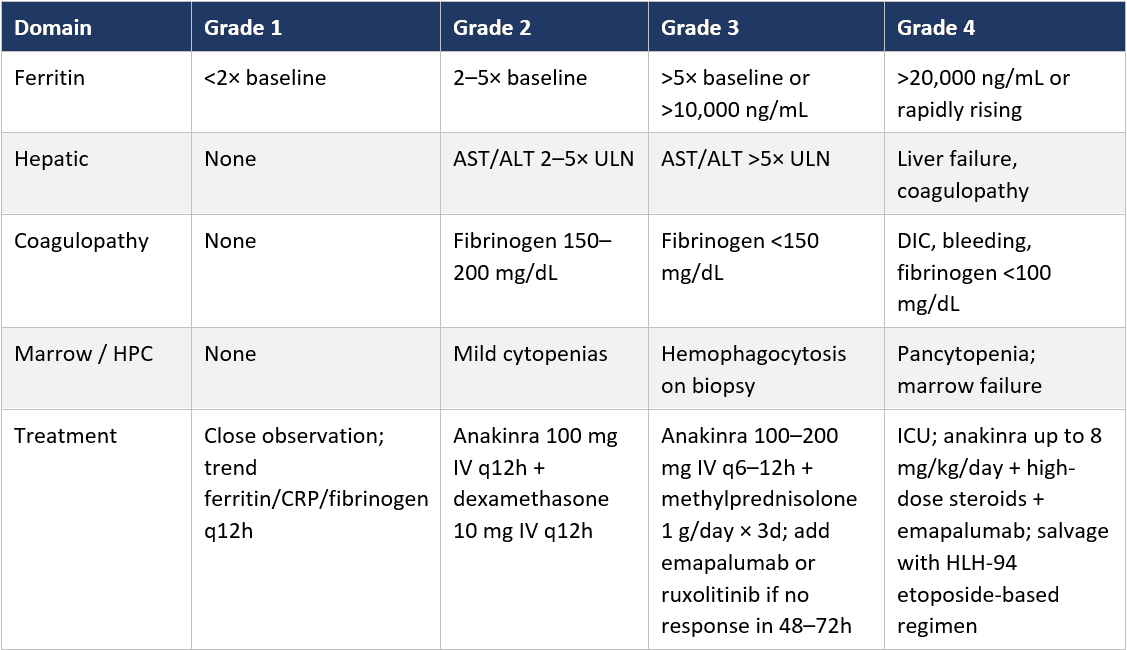
Table 4. Immune Effector Cell-Associated Encephalopathy (ICE) Score
A 10-point bedside test designed for rapid serial reassessment of CAR-T patients. Administration takes approximately 30 seconds. The Cornell Assessment of Pediatric Delirium (CAPD) is used for patients younger than 12 years.
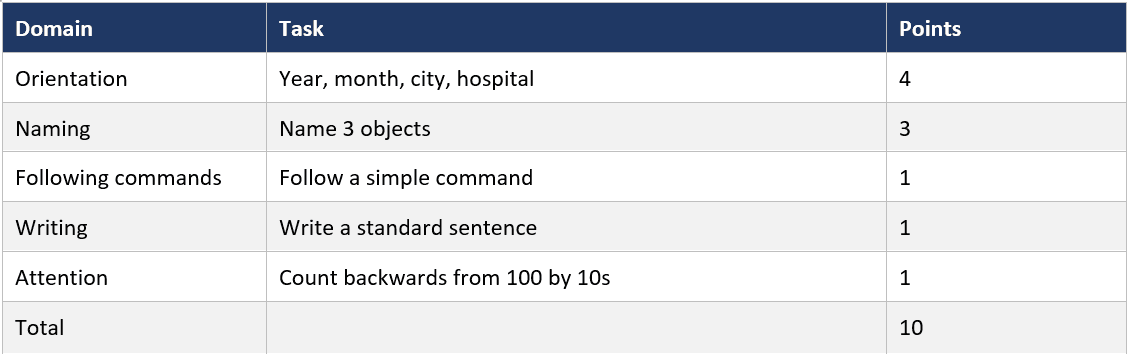
Table 5. ASTCT 2019 ICANS Grading and Management
Grade is set by the worst single domain across ICE score, level of consciousness, seizures, motor findings, and intracranial pressure/cerebral edema. Two findings auto-grade to 4 regardless of ICE score: deep focal weakness or decerebrate/decorticate posturing, and cerebral edema on imaging. Tocilizumab is NOT effective for isolated ICANS — dexamethasone is the cornerstone.
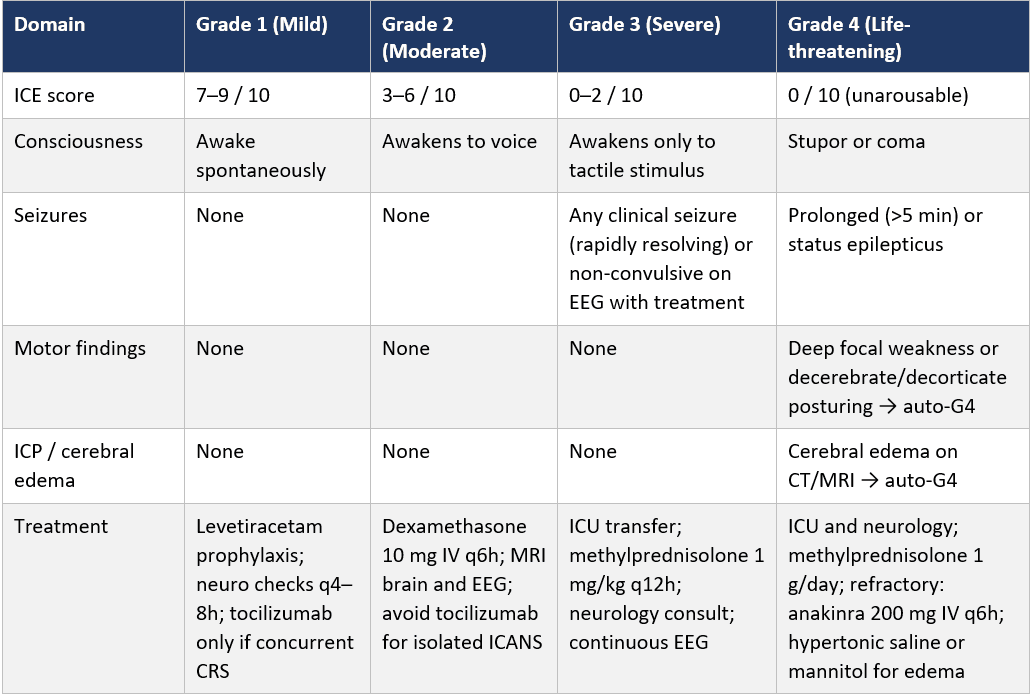
Table 6. Early ICAHT (Day 0–30): EHA/EBMT 2023 Grading and Management
Immune effector cell–associated hematotoxicity (ICAHT) is the dominant long-tail toxicity. Early ICAHT is set by ANC nadir and the duration spent below 500/μL. Three recovery phenotypes are recognized: quick recovery by day 21, intermittent with a second dip around day 14, and aplastic — the highest-risk pattern.
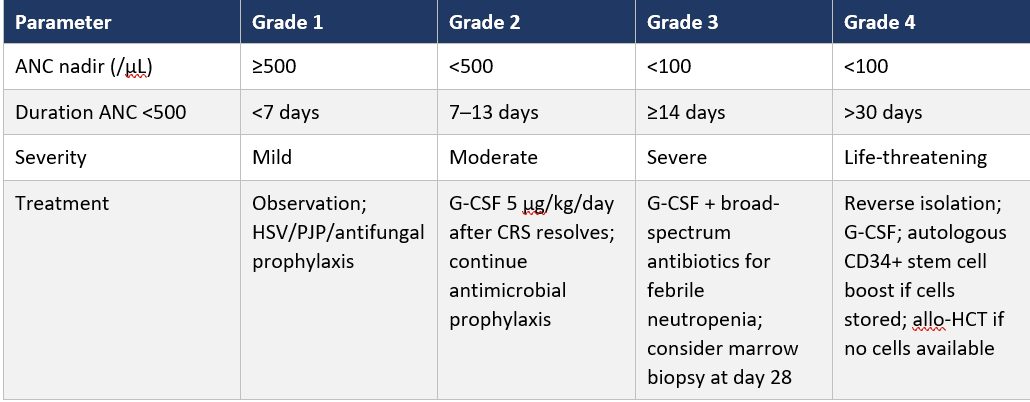
Table 7. Late ICAHT (After Day 30): EHA/EBMT 2023 Grading and Management
After day 30, the worst lineage sets the grade. Neutrophils, platelets, and hemoglobin are scored independently. Grade 4 aplastic ICAHT lasting beyond 30 days warrants strong consideration of an autologous CD34+ stem cell boost — which is the definitive intervention.
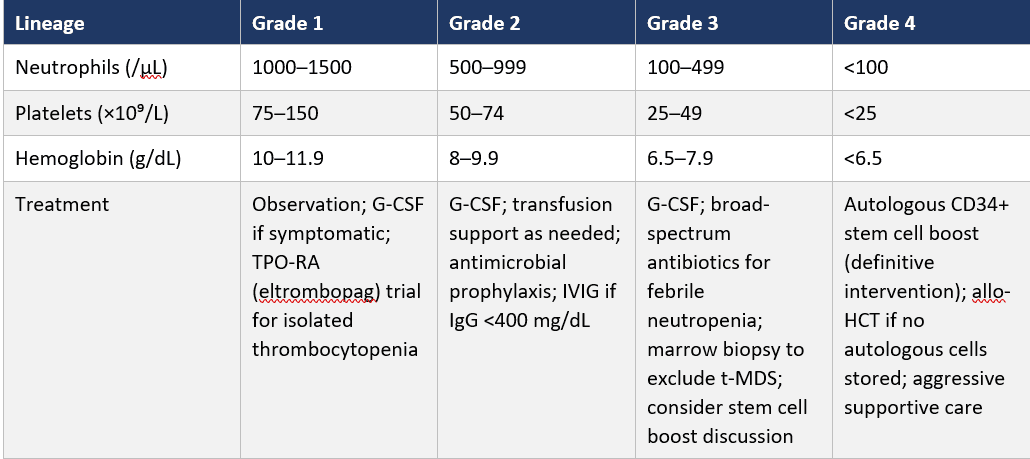
Table 8. Phase-Based Infection Risk After CAR T-Cell Therapy
Infection risk reflects a multilayered immune defect — lymphodepletion, B-cell aplasia, hypogammaglobulinemia, prolonged neutropenia, and steroid- and tocilizumab-related T-cell dysfunction. The intermediate and late phases are typically community-managed.
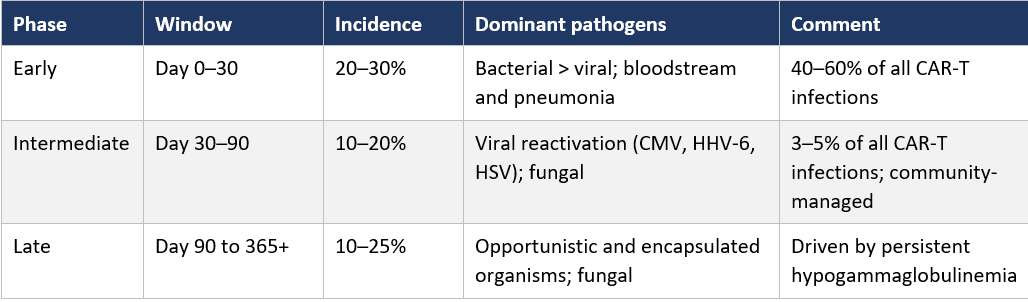
Table 9. Non-ICANS Neurotoxicity: Late Friendly-Fire Syndromes
These long-tail neurologic syndromes emerge weeks to months after infusion, well past the ICE-score window. They are not captured by ICE scoring and require a separate long-term monitoring framework. A normal ICE score in a patient with new gait disturbance, cranial nerve findings, or progressive cognitive change after BCMA CAR-T is not reassurance.
Supplementary tables for "What Every Oncologist Needs to Know About CAR-T Toxicity," originally presented at the Binaytara Cellular Therapy Symposium 2026, Session 5: Cellular Therapy for Community Practice.