Understanding Nepal’s Cancer Burden: Insights from a 15-Year Systematic Review
Key Insights
- Nepal currently lacks a pooled national estimate of its cancer burden. Existing data are fragmented across individual studies, hospital-based registries, and government reports, leaving cancer control programs without a comprehensive evidence base.
- Cancer accounts for approximately 10% of all deaths in Nepal. The mortality-to-incidence ratio is 0.6 which is higher than the global average of 0.52 suggesting late-stage diagnosis and limited access to treatment.
- Approximately 87% of gastrointestinal cancers in Nepal are diagnosed at stage III or IV, with a median time to diagnosis of about 150 days. In addition, 86.1% of patients experience financial hardship due to treatment costs.
- This PROSPERO-registered systematic review and meta-analysis conducted in accordance with PRISMA 2020 guidelines, synthesizes 15 years (2010-2024) of peer-reviewed cancer research conducted in Nepal. A total of 64 studies has been identified as eligible with manuscript submission targeted for July-August 2026.
- Breast cancer incidence in Kathmandu is estimated to be eight times higher than in remote districts highlighting significant urban-rural disparities in detection and diagnosis.
Why Nepal Lacks a National Cancer Burden Estimate
Nepal, a low- and middle-income country with a population of approximately 30 million, lacks a comprehensive synthesis of its national cancer burden. Data on cancer incidence, mortality, prevalence, and survival remain fragmented across individual studies, hospital-based registries, and government reports that were not originally designed to produce an integrated national estimate. Consequently, no pooled national cancer burden estimate currently exists. This gap has significant policy implications. Without reliable national evidence, cancer control programs cannot be efficiently targeted or prioritized. Policymakers lack the information necessary to identify where the burden is greatest and which populations are most affected.
To address this deficit, Dr. Roshan Kumar Mahato of the College of Medical Sciences at Kathmandu University, Professor Sujan Babu Marahatta, director of Nepal's Medical Education Commission and Dr. Kyaw min Htike, DrPH, Khon Kaen University is conducting a systematic review and meta-analysis synthesizing 15 years of peer-reviewed cancer research in Nepal between 2010 and 2024. The study is registered with PROSPERO and follow PRISMA 2020 reporting guidelines alongside a scoping review methodology.
Cancer Epidemiology in Nepal: Incidence, Mortality, and Risk Factors
Cancer accounts for approximately 10% of total deaths in Nepal and 5.6% of Disability-Adjusted Life Years (DALYs) according to Global Burden of Disease estimates. Nepal’s mortality-to-incidence ratio of 0.6 exceeds the global average of 0.52, indicating that delayed diagnosis and limited access to treatment contribute substantially to cancer mortality (Figure 1). The most common cancers reported in Nepal include cervical cancer (approximately 19%), lung cancer (approximately 17%), stomach cancer, and breast cancer. Tobacco use (both smoking and chewing) combined with alcohol consumption is associated with more than a 13-fold increase in cancer risk. Additional risk factors include household air pollution from biomass fuel use, rapid urbanization, dietary transitions, physical inactivity, and low screening uptake for breast and cervical cancers.
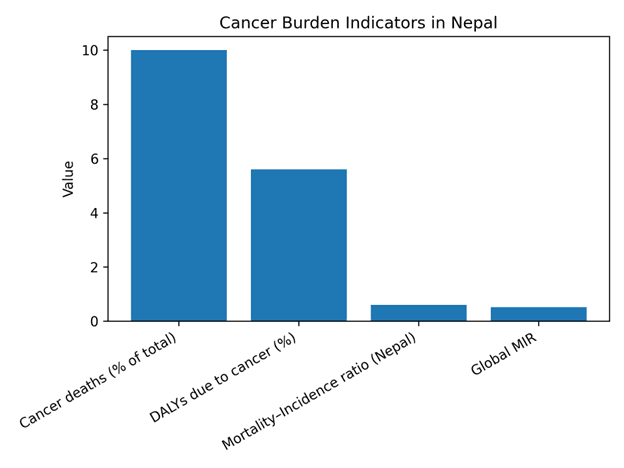
Figure 1. Cancer burden indicators in Nepal based on published estimates
Urban–Rural Disparities in Cancer Detection and Outcomes
Even within the currently available data, geographic disparities are pronounced. Urban cancer incidence is estimated to be 1.6 times higher among males and 1.9 times higher among females compared with rural populations such as those in Rukum (Figure 2). Breast cancer incidence in Kathmandu is reported to be approximately eight times higher than in remote districts. These differences reflect both increased exposure to urban lifestyle risk factors and improved diagnostic capacity in urban areas, whereas many rural cancer cases remain undetected or unreported.
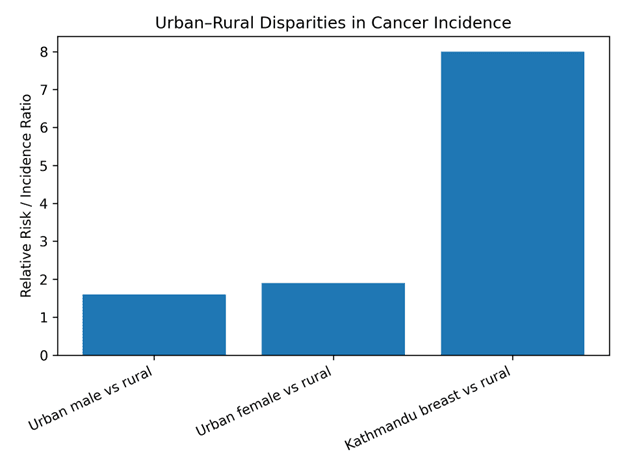
Figure 2. Urban-rural disparities in cancer incidence reported in the literature
The Impact of Late Diagnosis on Cancer Outcomes
The consequences of Nepal's fragmented cancer surveillance infrastructure are substantial. Screening coverage for cervical cancer remains extremely limited with uptake estimated at only 6.5%. Furthermore, only about 17% of health facilities have trained providers and established screening guidelines (Figure 3). Late-stage diagnosis is therefore common. Approximately 87% of gastrointestinal cancers are diagnosed at stage III or IV, with a median delay of approximately 150 days from symptom onset to diagnosis. At these stages, curative treatment options are often limited.
Financial Toxicity of Cancer Care in Nepal
The financial consequences for patients are also severe. Among individuals diagnosed with cancer, approximately 86.1% experience financial hardship related to treatment costs. Around 72% of patients report taking loans to cover expenses and 47% report selling property. The median direct cost is estimated at approximately USD 3,000 (around 346,000 Nepali rupees), representing a catastrophic financial burden for many households. Thus, cancer in Nepal represents not only a major health challenge but also a significant driver of household economic hardship.
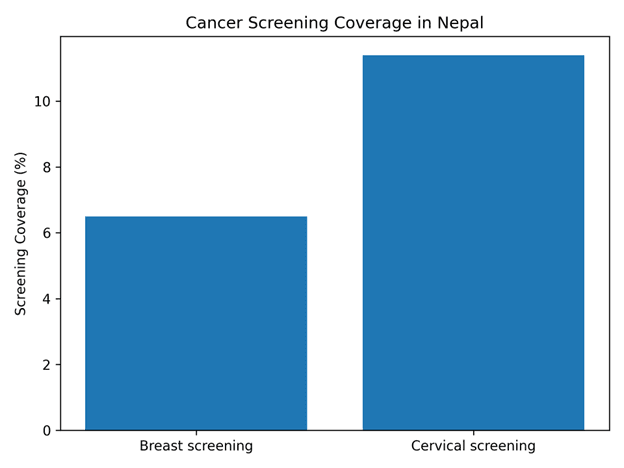
Figure 3. Cancer screening coverage for breast and cervical cancer in Nepal
Study Design and Methodology: PRISMA and PROSPERO Framework
The study applied a Population-Outcome (PO framework) targeting individuals diagnosed with cancer in Nepal. Analyses will be disaggregated by age, sex, geographic region, and ethnicity. Exposures of interest include environmental, lifestyle, genetic, and sociodemographic factors. Outcome include cancer incidence, prevalence, mortality, survival rates, healthcare access, and screening utilization across major cancer types including lung, breast, cervical, stomach, and head and neck cancers.
Database searches conducted in PubMed, Scopus, and CINAHL identified 224 records. After deduplication and independent title and abstract screening by four to five researchers, 135 full-text articles were assessed for eligibility. As of Binaytara's Spring Research Day 2026, 64 studies had been confirmed eligible for quality assessment, 35 had been excluded, and 36 remained under discussion pending consensus review (Figure 4).
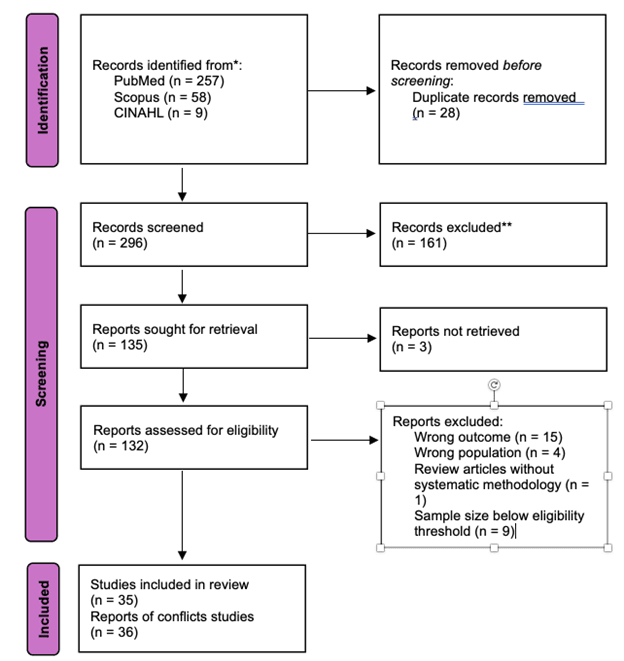
Figure 4. PRISMA flow diagram showing the screening process for studies included in the systematic review
Quality Assessment and Statistical Approach
For cross-sectional studies, an eight-item critical appraisal tool is applied to evaluate inclusion criteria clarity, exposure measurement validity, description of participants and settings, identification of confounding factors and statistical methodology. Studies scoring 7 to 8 points proceed to meta-analysis. Moderately scoring studies are included with noted limitations while studies scoring below 3 are restricted to narrative synthesis. For cohort and case-control studies, a seven-item assessment tool evaluates confounding control, participant selection, exposure classification, handling of missing data, outcome measurement validity, and repeated measurement concerns. Articles are categorized as having low, moderate, serious, or critical risk of bias.
Statistical analyses will be conducted using R. Random effects models will be applied for heterogeneous datasets while fixed effects models will be used for homogeneous groups. Funnel plots will be used to assess publication bias. Planned subgroup analyses will stratify findings by cancer type, sex, age group, geographic location (urban versus rural and remote regions), study period (2010-2015 and 2016-2024), and risk factor categories. Geographic information systems (GIS) cluster analysis will also be conducted to map cancer burden hotspots relative to the distribution of oncology services. As this systematic review and meta-analysis is currently in progress, the findings presented here reflect the existing literature and study progress rather than final pooled estimates.
Phase Two Research and Policy Implications for Nepal
The second phase of study will incorporate additional primary data sources including administrative cancer incidence and mortality trends across Nepal's districts, GIS-based cluster analysis, key informant interviews with oncologists, policymakers, and healthcare providers, and focus group discussions with cancer patients and community members. This mixed-methods approach will help to identify policy gaps in cancer prevention, screening and treatment.
Expected outputs include a peer-reviewed manuscript targeted for submission by July or August 2026, and a policy brief for Nepal's Ministry of Health and Population, the World Health Organization, and NGO partners. The findings are intended to inform Nepal's National Cancer Control Strategy (2024-2030), support expansion of screening infrastructure, and strengthen the evidence base for establishing additional cancer treatment centers. The research team includes Associate Professor Dr. Roshan Kumar Mahato, Professor Sujan Babu Marahatta, a US-based research team, and student researchers from Kathmandu University and Pokhara University.
Conclusion: Building a National Cancer Control Strategy for Nepal
Nepal’s cancer burden continues to rise, yet the national evidence base remains fragmented. By synthesizing fifteen years of research, this systematic review aims to provide the first comprehensive national assessment of cancer incidence, mortality, and associated risk factors in Nepal. Such evidence is essential for guiding screening expansion, strengthening treatment infrastructure, and supporting the development of effective national cancer control strategies.
Frequently Asked Questions About Cancer Burden in Nepal
Why doesn't Nepal already have a national cancer burden estimate?
Nepal's cancer data is fragmented across individual studies, hospital-based registries, and government reports not designed for integration. There is no national cancer registry with adequate geographic and demographic coverage. This systematic review is the first effort to synthesize 15 years of peer-reviewed data into a comprehensive national picture.
What are the most common cancers in Nepal?
Cervical cancer (approximately 19%), lung cancer (approximately 17%), stomach cancer, and breast cancer. Tobacco-related cancers account for 35.3% of all male cancers.
How severe is late-stage diagnosis in Nepal?
87% of gastrointestinal cancers are diagnosed at stage III or IV, with a median time to diagnosis of approximately 150 days. By this point, curative treatment options are severely limited.
What is the financial impact of cancer treatment in Nepal?
86.1% of patients face financial hardship; 72% take out loans, 47% sell property. The median direct treatment cost is approximately USD 3,000 — a catastrophic burden for most Nepali households.
When will the study be published?
The systematic review and meta-analysis manuscript is targeted for submission by July or August 2026. Phase two primary data collection and policy analysis will follow.