Reaching Out-of-School Maasai Girls With HPV Vaccination: A Community-Led Model for Cervical Cancer Prevention in Tanzania
Out-of-school girls in Tanzania’s Maasai communities face a critical gap in cervical cancer prevention. A new community-led HPV vaccination model aims to close this divide—bringing life-saving vaccines directly to those historically left behind.
Key Insights: Closing the Cervical Cancer Prevention Gap in Maasai Communities
- School-based HPV vaccination programs in Tanzania systematically exclude out-of-school girls in Maasai communities, a structural equity gap that this pilot project is designed to close.
- The single-dose HPV vaccine, available free through public health channels, eliminates the need for follow-up appointments and is uniquely suited to nomadic and semi-nomadic lifestyles.
- The delivery model relies on two existing community structures: trained community healthcare workers and Maasai Mamas—respected elder women whose social authority is central to mobilizing families.
- The pilot, launching in April 2026, targets coverage of at least 60% of eligible out-of-school girls and aims to produce a scalable model for other pastoralist communities across Tanzania and the region.
- Building community healthcare worker capacity to discuss cervical cancer and non-communicable diseases is a core secondary objective of the program.
Understanding the Structural Gap in Tanzania’s HPV Vaccination Program
National HPV vaccination programs in Tanzania and across sub-Saharan Africa are delivered primarily through school-based platforms. This design is efficient within its parameters, but it creates a well-defined and measurable equity gap: girls who are not enrolled in formal education receive neither the vaccine nor the accompanying health literacy that school-based programs provide.
In Maasai communities in northern Tanzania, the problem is particularly acute. Nomadic and semi-nomadic lifestyles, early marriage, and traditional gender norms mean that a significant proportion of eligible girls never enter the school system. This population faces substantially higher cervical cancer risk without access to the primary preventive intervention that could reduce it. The cervical cancer equity deficit between in-school and out-of-school female populations is not incidental; it is a structural consequence of a delivery model that was not designed to reach them.
A parallel challenge involves community healthcare workers, who in Tanzania, as in many low- and middle-income countries, are trained and resourced primarily through infectious disease programs. These workers are knowledgeable and trusted in their communities when it comes to HIV, tuberculosis, and malaria. Many, however, lack the vocabulary, training, and confidence to discuss non-communicable diseases, including cancer. Closing this knowledge gap is a central objective of the pilot project led by Dr Innocent H. Peter Uggh of the Kilimanjaro Clinical Research Institute (KCRI) in Moshi, Tanzania.
A Logistical Breakthrough: How the Single-Dose HPV Vaccine Enables Community-Based Delivery
A critical enabling factor for community-based HPV delivery is the availability of the single-dose HPV vaccine, provided free of charge through Tanzania's public health system. The earlier two-dose schedule required a follow-up appointment, a logistical barrier that is prohibitive for families who move seasonally across grazing territories. A missed second dose meant no protection.
The single-dose regimen fundamentally changes this equation. A single contact with a healthcare worker provides full protection, making community-based delivery genuinely feasible for the first time for nomadic populations. The logistical compatibility of the single-dose vaccine with nomadic lifestyles is not merely convenient; it is the prerequisite that makes the entire program architecture possible.
Community-Driven Delivery: The Role of Maasai Mamas and Healthcare Workers
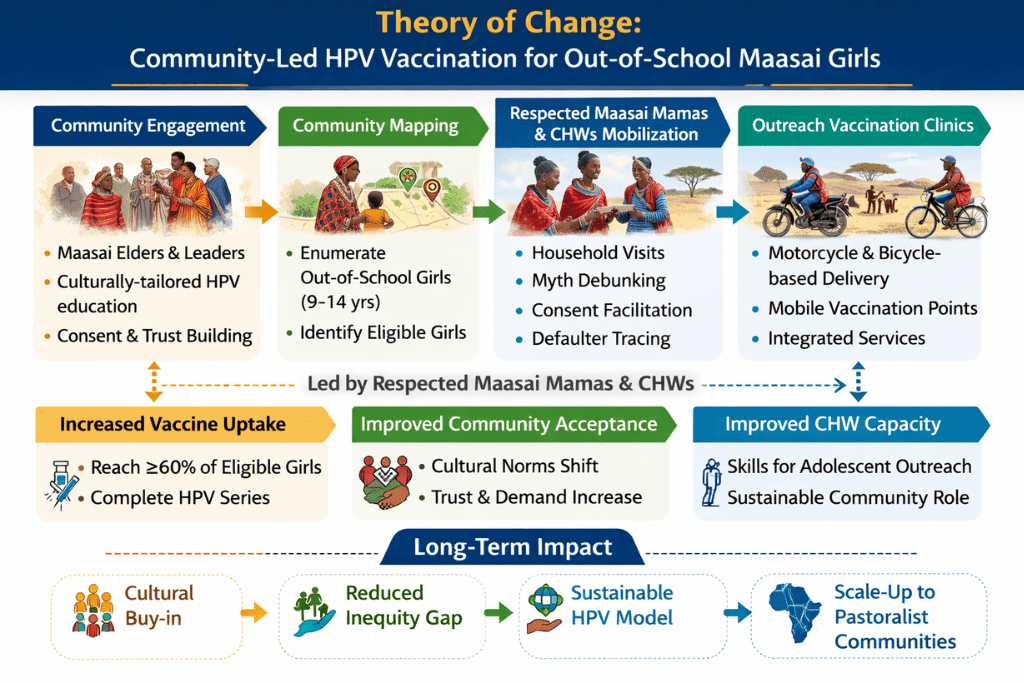
The program's delivery model is built on two interlocking community structures that already exist and already command trust within Maasai communities. The first is Tanzania's community healthcare worker (CHW) system. Many of Tanzania's CHWs have received years of formal training and are embedded in the communities they serve. This program will train them to speak confidently about HPV vaccination and cervical cancer, adding non-communicable disease competency to the infectious disease knowledge that currently defines their scope.
The second structure is the institution of the Maasai Mama: older, respected women in Maasai communities who hold significant social authority, particularly in matters affecting younger women and girls. Maasai Mamas will be trained to identify eligible out-of-school girls, communicate the purpose and importance of the HPV vaccine to girls and their families in culturally appropriate terms, and mobilize them to a community location where a CHW can administer the vaccine, eliminating the requirement for a health facility visit entirely.
This model inverts the standard logic of facility-based vaccination delivery. Rather than requiring girls to come to the health system, the health system comes to them.
Study Design: A Community-Based Implementation Approach
The project, funded in part by the American Cancer Society through Cervical Cancer Action for Elimination, is designed as a community-based mixed-methods implementation study beginning in April 2026. Participants include out-of-school Maasai girls and their parents or guardians, Maasai Mamas, community healthcare workers, and local health providers.
The implementation sequence begins with meetings between the research team and community gatekeepers, Maasai elders, and community leaders whose endorsement is treated as a prerequisite for any subsequent outreach. This phase is followed by a structured assessment of barriers and knowledge gaps related to HPV vaccination within the target communities, with findings directly informing the design of training modules for both CHWs and Maasai Mamas.
Following training, Maasai Mamas identify and mobilize eligible girls while CHWs administer the vaccine at community locations. The program acknowledges the inherent uncertainty of working with a population whose historical engagement with formal health systems has been limited and deliberately centres community structures and voices as the foundation for earning and sustaining trust.
Expected Outcomes and Scalability Across Tanzania
The program's primary coverage target is to reach at least 60% of eligible out-of-school girls in the target communities. Secondary outcomes include measurable improvements in community-level knowledge and acceptance of HPV vaccination, a cadre of CHWs with demonstrated competency in discussing cancer prevention, and documented cultural buy-in from the Maasai community as evidence of program viability.
The ultimate objective extends beyond the pilot itself. The program is designed to generate a replicable, scalable delivery model that can be adapted for other out-of-school girl populations and pastoralist communities in Tanzania and the broader region. Planned publications will address barriers and facilitators to HPV vaccination in Maasai communities, implementation outcomes and lessons learned, and a policy brief on community-led vaccination delivery.
Building Sustainable Cancer Prevention Infrastructure in Africa
Dr Uggh also coordinates the Network of Oncology Researchers in Africa (NORA) project at the Kilimanjaro site, which supports cancer research capacity-building through postdoctoral, doctoral, and master's-level training. The HPV vaccination pilot reflects the same principle that underlies NORA: that closing the gap in cancer outcomes in sub-Saharan Africa requires investing in both community-level delivery and scientific infrastructure simultaneously.
Frequently Asked Questions About HPV Vaccination in Maasai Communities
Why do out-of-school girls in Maasai communities face higher cervical cancer risk?
Tanzania's national HPV vaccination program is delivered through schools, so girls who are not enrolled in formal education receive neither the vaccine nor the health education associated with it. In Maasai communities, nomadic lifestyles, early marriage, and traditional gender roles interrupt schooling for a significant proportion of eligible girls, creating a direct and measurable prevention gap.
What makes the single-dose HPV vaccine particularly important for this program?
The single-dose vaccine requires only one contact with a healthcare worker for full protection, eliminating the need for a follow-up appointment. This is critical for nomadic families who cannot reliably return to a fixed location for a second dose. The single-dose regimen is what makes community-based delivery to this population logistically feasible.
Who are Maasai Mamas, and what role do they play?
Maasai Mamas are respected elder women within Maasai communities whose social authority makes them trusted agents of health promotion. In this program, they are trained to identify eligible out-of-school girls, communicate the purpose and safety of the HPV vaccine to families, and coordinate with community healthcare workers to arrange vaccination at community locations rather than health facilities.
What is the target vaccination coverage rate for this pilot?
The program targets coverage of at least 60% of eligible out-of-school girls in Monduli during the pilot phase beginning April 2026.
What happens after the pilot?
The program is designed from the outset to produce a replicable model. Planned outputs include peer-reviewed publications on barriers and facilitators, implementation outcomes, and a policy brief intended to inform national vaccination strategy and support adaptation of the model for other pastoralist communities in Tanzania and the region.