This article was reviewed for accuracy by Wade Swenson, MD, MPH, MBA, on 6/20/2026.
Rural Cancer Care and the Dollar Sign on Your Diagnosis
In Juneau, Alaska — a city of 30,000 — there is not a single oncologist. When Beth Comstock was diagnosed with stage 4 breast cancer, she flew to Seattle for treatment, spending thousands of dollars and closing out her retirement fund. Her story is not an anomaly. It is a window into the structural, financial, and policy failures that define rural cancer care across the United States.
Who Can Afford Cancer?
When Beth Comstock was diagnosed with breast cancer, her primary care physician told her: “I am in over my head. I don’t know what to do.”
Comstock lives in Juneau, Alaska’s state capital. The city is home to over 30,000 people—but not a single oncologist. Alaska’s statewide oncology capacity doesn’t inspire much more optimism: there are 19 oncologists in the entire state [1], concentrated in the more populous Fairbanks and Anchorage. “Those of us who live anywhere else have to rely on clinics,” Comstock explained: “in my case, a radiologist and a pathologist who wasn't used to doing breast cancer tissue, and staged me as 2B.” She was stage 4.
That was when her PCP referred her to receive care out of state, in the Seattle-based Swedish Cancer Institute. In Seattle, with a population exceeding that of the entire state of Alaska, the oncology landscape is remarkably different. A regional registry lists over 500 oncologists in the metropolitan area [2]. The city has an array of dedicated cancer centers (the largest of which employs over 100 medical oncologists alone [3]), or specialty teams within larger hospital systems. Either way, it’s a far cry from Juneau’s clinic-dominated model.
Seattle’s Swedish Cancer Institute had the depth of care Comstock’s metastasized cancer required, but at a price: around a thousand dollars a plane ticket. In Comstock’s first month receiving out-of-state treatment, she traveled from her home in Juneau to her care team in Seattle three times. After that first month, she averaged a thousand-dollar flight once every three months.
Comstock racked up so many airline miles during her treatment that she and her family went to Hawaii. “That was the lemonade in it,” she reflected wryly. “Breast cancer sent me and my family on vacation.”
Still, Comstock had to close out her retirement fund to pay off the credit cards that allowed her to travel to and from Seattle. She considers herself lucky. “I am upper-middle class. Thankfully, I have extremely good insurance that covers me at $19,811 every 28 days, with no out-of-pocket for me. But how many other patients aren't getting the same chance I've got, because they don't have the money or the access or the fight I've had?”
Interconnected Issues: Rural and Financial Cancer Care Barriers
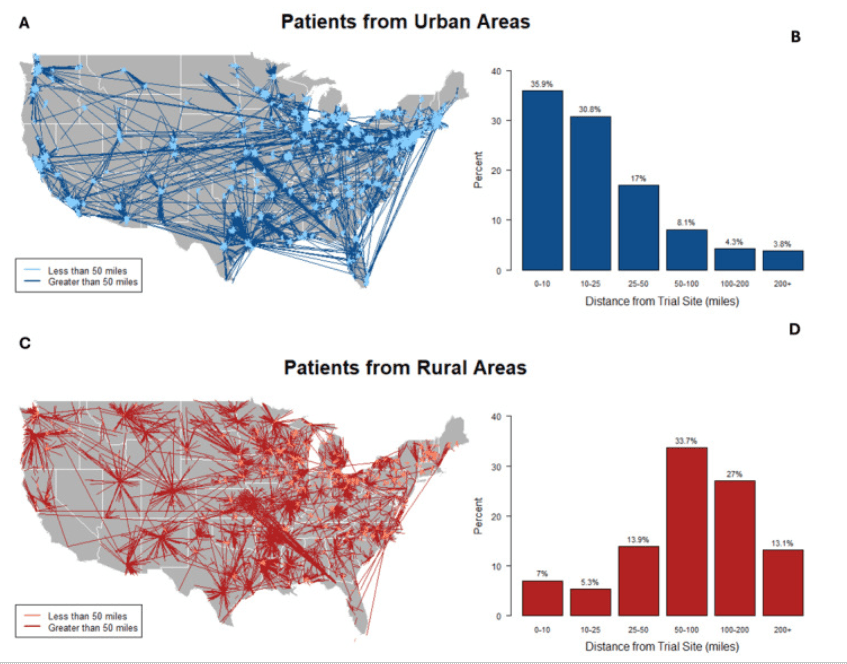
Figure 1: Distance from clinical trial site for urban vs. rural patients. Reposted from https://pmc.ncbi.nlm.nih.gov/articles/PMC12223359/.
Rural cancer incidences are associated with higher rates of morbidity and mortality compared to urban cancer incidences [4]. Even as clinical trials and FDA approvals improve outcomes across the board, cancer mortality is falling more slowly in rural areas of the United States [5]. There is less access to state-of-the-art prevention, diagnosis, and treatment services; there are fewer PCPs and specialists, and a higher rate of physician turnover [5]. Higher rates of risk factors like smoking and obesity point to a fundamental failure within preventive services.
Yet geography doesn't mean inherent unhealthiness: when rural cancer patients participate in clinical trials, they experience equivalent outcomes to urban cancer patients in the same trials [5]. Rural patients are simply less likely to be invited to participate, and less likely to participate if invited [5]. There is a rural cancer survival disparity: where you live impacts your odds of surviving cancer.
Wade Swenson, MD, MPH, MBA, oncologist-hematologist at Lakewood Health System in Staples, Minnesota, and co-founder of the Rural Cancer Institute, weighed in for The Cancer News.
“Alaska starkly illustrates how geographic isolation affects cancer outcomes, with a limited oncology workforce, long travel distances, and a predominantly Indigenous patient population facing historical underinvestment in care infrastructure,” Swenson said. Observed disparities are correlated with degree of isolation (and, as Swenson alludes to, exacerbated in ethnic minority populations) [4], so a remote area like Alaska offers a neatly illustrated case study.
As Comstock highlighted, many of these rurality-associated barriers are inexorably tied with financial burden. If you live somewhere that doesn’t have access to appropriate treatment services, it costs money to travel to an urban hub that does. This is an issue, then, that begins on the level of infrastructure, not patient care. According to tracking data from the University of North Carolina's Sheps Center, there have been 154 rural hospital closures since 2010 [4]. There are financial barriers on both the patient and provider sides of rural cancer care.
What does a world with equitable access to state-of-the-art treatment look like, and what does it take to get there? As Swenson sees it, the solution—or at least the roadmap to a solution—spans workforce, policy, and education.
Workforce: The Directly Employed Oncologist Model
“The directly employed rural oncologist model, in which a community hospital hires an oncologist as a permanent member of its medical staff rather than using traveling specialists, is the structural solution…” Swenson said. “It keeps the oncologist embedded in the community, builds trust over time, and keeps care more local.” Given that rural communities like Juneau lack a permanent residing specialist, implementing an accessible program with a permanent oncologist “is the most durable approach I've seen,” Swenson said.
Juneau had no permanently employed oncologist, exactly the infrastructure gap Swenson's directly employed model is designed to close.
The benefits are documented. In the remote mountainous town of Truckee, CA, a team established a hospital after observing that residents traveled significant distances to receive primary and secondary care in midsized cities [6]. With severe disease burdens, tertiary and even quaternary care was necessary at increasingly specialized cancer centers across the state [6]. A decade after initial implementation, the center had seen around 100 patients a year with positive feedback, the team had brought on a second directly employed oncologist, and they were looking to open a second center.
That implementation was supported in part by UC Davis. This points to a larger concern about the financial viability of independent rural cancer programs, and raises the question: which federal policies are necessary to make the model sustainable in the long term?
Policy: Critical Access Hospitals
According to Swenson, one of the most “actionable federal levers right now” is “Critical Access Hospital designation and its associated cost-based reimbursement, which is what makes it financially viable for systems like mine to directly employ an oncologist rather than rely on itinerant coverage.”
Eligible rural hospitals can be designated Critical Access Hospitals (CAH). This status confers certain financial benefits (namely cost-based reimbursement for Medicare services) that promote long-term financial viability for these institutions, ensuring remote locations have access to essential services [7]. CAH designation can be the difference—and is the difference, in Swenson’s experience—between a rural hospital employing a permanent oncologist or not.
Even with this protection, the urban-rural cancer health disparity is widening, and the protection itself is more tenuous than Swenson would like. The Center for Medicare & Medicaid Services (CMS) has generated unrest among rural oncology stakeholders by revoking CAH status based on mileage recalculations. The affected hospital’s status has since been restored—but the apparent fragility of the CAH designation is not to be ignored.
The Positive: Education and Telehealth
The reality is this: CAH designation is an important stepping stone to rural cancer health equity, not the end of the road. Swenson is actively involved in advocacy work in the space—but contesting a policy reversal prevents an equity backslide; it doesn’t make diagnoses like Comstock’s any easier. To this end, Swenson introduced his final pillar of rural oncology viability and sustainability: rural cancer care education.
“The thesis is simple,” Swenson said: “students who train in rural areas are more likely to practice in rural areas.” This thesis underlies Rural Cancer Institute’s CORE (Clinical Oncology Rural Experience) program, “which exposes trainees to rural oncology practice and cultivates the next generation of rural cancer physicians,” Swenson explained.
Where policy works backward from an existing gap, Rural Track Programs like CORE lay the foundation for a capable and stable future rural health sector. CORE inspires and prepares (as RCI’s website differentiates [8]) medical students, residents, fellows, physician assistants, and nurse practitioner students to practice in rural settings. The benefit of such programs is documented in the broader health space. Rural residency training is a strong predictor of rural practice, one study found, concluding that “[i]ncreasing rural programs for training residents from both rural and urban backgrounds, as well as recruiting more rural students to medical education, could increase the number of rural family physicians” [9]. CORE responds to this call to action in the oncology space.
While oncology Rural Track Programs begin the years-long educational process, Swenson points to telehealth—the use of communications technology to support long-distance healthcare—as an important here-and-now tool. Tele-oncology, or technology-enabled long-distance cancer care, has, according to one survey, a high satisfaction rate and significant, documented clinical benefits [10]. But its policy footing remains unstable.
A Brief History of Telehealth
During the COVID-19 public health emergency (PHE), Medicare expanded their coverage of telehealth. What before had been a service- and location-restricted premium became a widely supported mainstay appointment format [11]. The waiver on telehealth restrictions was set to expire as the pandemic waned. Yet post-PHE, telehealth use remains nearly two times higher than before 2019, leading to several extensions of the expanded coverage, the most recent of which goes through December 2027 [11]. Given the benefits, advocates posit that a permanent extension of telehealth coverage is warranted.
Advocacy, then, is a necessary avenue for structural change. Along with CAH designation, Swenson, who has “testified on these issues before the Minnesota Legislature and contributed to ASCO's policy work in this space,” sees permanent Medicare telehealth expansion as one of the most important policy areas in rural cancer care equity.
The Non-Exhaustive Beginner’s Guide to Getting Involved
For oncologists and healthcare professionals: ASCO's ACT Network offers pre-drafted advocacy letters and an annual two-day Advocacy Summit. AMA has similar programs. The Physicians Grassroots Network provides a legislator search tool and bill tracker for those without membership. Patient stories are consistently among the most effective tools with policymakers, and CancerNation's annual Survivorship Survey is one avenue for contributing yours.
For patients: Rural Cancer Institute has compiled a range of individual resources. Bright Spot Network's Bright Grants offer financial assistance to caregivers of children under six; Vital Options International provides relief for those with rare diseases (including cancer) facing financial hardship. ClinicalTrials.gov allows patients to browse trials by location and eligibility criteria. Participating is one way to access cutting-edge treatment while contributing to the evidence base.
The Other Side
Beth Comstock is, in her words, “a stage four thriver. I've now had two PET scans that showed no metabolic activity at all.”
She was also, in her words, lucky: not a likely descriptor for someone with stage 4 breast cancer—but given the cancer care infrastructure associated with her zip code, not an inaccurate one. To acknowledge that Beth Comstock is lucky is to throw into relief the unfairness of rural cancer care. How much longer will we accept that luck is a factor in cancer treatment?
References
- Statista. "Number of active physicians in Alaska as of 2023, by specialty area." Statista, 2023. https://www.statista.com/statistics/209433/number-of-active-physicians-in-alaska-by-specialty-area/
- U.S. News & World Report. "Oncologists in Seattle, WA." U.S. News Health. https://health.usnews.com/doctors/oncologists/washington/seattle
- Fred Hutchinson Cancer Center. "Provider Directory." https://www.fredhutch.org
- Unger JM, McAneny BL, Osarogiagbon RU. Cancer in rural America: Improving access to clinical trials and quality of oncologic care. CA Cancer J Clin. 2025;75(4):341-361. doi:10.3322/caac.70006
- Bhatia S, Landier W, Paskett ED, et al. Rural-Urban Disparities in Cancer Outcomes: Opportunities for Future Research. J Natl Cancer Inst. 2022;114(7):940-952. doi:10.1093/jnci/djac030
- Heifetz LJ, Christensen SD, Devere-White RW, Meyers FJ. A model for rural oncology. J Oncol Pract. 2011;7(3):168-171. doi:10.1200/JOP.2010.000167
- Rural Health Information Hub. "Critical Access Hospitals." https://www.ruralhealthinfo.org/topics/critical-access-hospitals
- Rural Cancer Institute. "CORE Program." https://www.ruralcancer.org/core
- Patterson DG, Shipman SA, Pollack SW, et al. Growing a rural family physician workforce: The contributions of rural background and rural place of residency training. Health Serv Res. 2024;59(1):e14168. doi:10.1111/1475-6773.14168
- Lopez AM. Telehealth in Cancer Care: Inequities, Barriers, and Opportunities. Cancer J. 2024;30(1):2-7. doi:10.1097/PPO.0000000000000694
- KFF. "What to Know About Medicare Coverage of Telehealth." KFF, 2025. https://www.kff.org/medicare/what-to-know-about-medicare-coverage-of-telehealth/